
SUMMARY: The American Cancer Society estimates that 59,340 people will be diagnosed with Head and Neck cancer in 2015 and 12,290 patients will die of the disease. Patients with recurrent/metastatic Squamous Cell Carcinoma of the Head and Neck (SCCHN) have a poor prognosis with a median Overall Survival (OS) of about 13 months with first line therapy and about 6 months or less with later lines of therapy. The treatment paradigm for solid tumors has been rapidly evolving with a better understanding of the Immune checkpoints. Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent, related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4), also known as CD152, PD-1(Programmed cell Death-1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. The first Immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® (Ipilimumab), an antibody that blocks Immune checkpoint protein/receptor CTLA- 4, has been shown to prolong overall survival in patients with previously treated, unresectable or metastatic melanoma. KEYTRUDA® (Pembrolizumab) is a fully humanized, Immunoglobulin G4, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the tumor-specific effector T cells. The FDA granted accelerated approval to KEYTRUDA® in September 2014, for the treatment of patients with unresectable or metastatic melanoma and disease progression following YERVOY® and, if BRAF V600 mutation positive, a BRAF inhibitor. The activity of KEYTRUDA® as a single agent in advanced SCCHN patients, was previously published and was noted in PD-L1 positive tumors, regardless of the Human PapillomaVirus (HPV) status. The Overall Response Rate in this patient group was 20% and 29% of patients had stable disease. The authors in this study reported the efficacy of once every three week dose of KEYTRUDA®, in a larger expansion cohort of KEYNOTE 012 study. In this study, 132 patients with recurrent/metastatic SCCHN were enrolled, regardless of their PD-L1 expression or HPV status. These patients received a fixed dose of KEYTRUDA® 200 mg IV, every 3 weeks and patients were evaluated every 8 weeks with radiographic imaging. The mean age was 59 years and 57% of the patients had 2 or more lines of therapy for recurrent disease. Treatment was continued until disease progression. The primary end point was Overall Response Rate (ORR) and secondary endpoints included Progression Free Survival (PFS) and Overall Survival (OS). The Overall Response Rate was 25% and stable disease was noted in an additional 25% of the patients. This amounted to a disease control rate of 50%. Patients with HPV-positive disease had a response rate of 20.6% and patients with HPV-negative disease had a response rate of 27.2%, suggesting that KEYTRUDA® was active in both subgroups of patients. Serious toxicities were reported in fewer than 10% of patients and the most common adverse event was fatigue (15.2%). The authors concluded that KEYTRUDA® given every 3 weeks was well tolerated and demonstrated a meaningful response rate in a heavily pretreated population of patients, with recurrent/metastatic SCCHN. Evaluation of PD-L1 status for this patient group is ongoing. Antitumor activity and safety of pembrolizumab in patients (pts) with advanced squamous cell carcinoma of the head and neck (SCCHN): Preliminary results from KEYNOTE-012 expansion cohort. Seiwert TY, Haddad RI, Gupta S, et al. J Clin Oncol 33, 2015 (suppl; abstr LBA6008)</s
Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent, related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system. Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4), also known as CD152, PD-1(Programmed cell Death-1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. The first Immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® (Ipilimumab), an antibody that blocks Immune checkpoint protein/receptor CTLA- 4, has been shown to prolong overall survival in patients with previously treated, unresectable or metastatic melanoma. KEYTRUDA® (Pembrolizumab) is a fully humanized, Immunoglobulin G4, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the tumor-specific effector T cells. The FDA granted accelerated approval to KEYTRUDA® in September 2014, for the treatment of patients with unresectable or metastatic melanoma and disease progression following YERVOY® and, if BRAF V600 mutation positive, a BRAF inhibitor. The activity of KEYTRUDA® as a single agent in advanced SCCHN patients, was previously published and was noted in PD-L1 positive tumors, regardless of the Human PapillomaVirus (HPV) status. The Overall Response Rate in this patient group was 20% and 29% of patients had stable disease. The authors in this study reported the efficacy of once every three week dose of KEYTRUDA®, in a larger expansion cohort of KEYNOTE 012 study. In this study, 132 patients with recurrent/metastatic SCCHN were enrolled, regardless of their PD-L1 expression or HPV status. These patients received a fixed dose of KEYTRUDA® 200 mg IV, every 3 weeks and patients were evaluated every 8 weeks with radiographic imaging. The mean age was 59 years and 57% of the patients had 2 or more lines of therapy for recurrent disease. Treatment was continued until disease progression. The primary end point was Overall Response Rate (ORR) and secondary endpoints included Progression Free Survival (PFS) and Overall Survival (OS). The Overall Response Rate was 25% and stable disease was noted in an additional 25% of the patients. This amounted to a disease control rate of 50%. Patients with HPV-positive disease had a response rate of 20.6% and patients with HPV-negative disease had a response rate of 27.2%, suggesting that KEYTRUDA® was active in both subgroups of patients. Serious toxicities were reported in fewer than 10% of patients and the most common adverse event was fatigue (15.2%). The authors concluded that KEYTRUDA® given every 3 weeks was well tolerated and demonstrated a meaningful response rate in a heavily pretreated population of patients, with recurrent/metastatic SCCHN. Evaluation of PD-L1 status for this patient group is ongoing. Antitumor activity and safety of pembrolizumab in patients (pts) with advanced squamous cell carcinoma of the head and neck (SCCHN): Preliminary results from KEYNOTE-012 expansion cohort. Seiwert TY, Haddad RI, Gupta S, et al. J Clin Oncol 33, 2015 (suppl; abstr LBA6008)</s
Month: June 2015
ASCO 2015 Selective Internal Radiation Therapy with Y-90 Improves Outcomes in Metastatic Colorectal Cancer
SUMMARY:The American Cancer Society estimates that approximately 133,000 new cases of ColoRectal Cancer (CRC) will be diagnosed in the United States in 2015 and close to 50,000 are expected to die of the disease. Approximately 15-25% of the patients with CRC present with metastatic disease at the time of diagnosis (synchronous metastases) and 50-60% of the patients with CRC will develop metastatic disease during the course of their illness. About 10-20% of the patients with liver metastases have resectable disease, which may translate into long term survival. CRC patients with synchronous metastases tend to have more extensive disease with bilobar liver involvement. With the availability of more effective chemotherapy regimens and targeted systemic interventions, the median survival of CRC patients with metastatic disease has increased from 6 months in the 1990’s to 24 months. Selective Internal Radiation Therapy (SIRT) or RadioEmbolization using radioisotope Yttrium-90 (Y-90) coated resin particles, a pure beta emitter, has demonstrated significant benefit for patients with unresectable liver metastases, in previously published studies. Y-90 resin microspheres are no bigger in diameter than a human hair and are introduced into the hepatic artery by initially accessing the femoral artery. The blood supply to the liver tumors is via the hepatic artery and these tumors tend to be hypervascular. The Y-90 resin microspheres become preferentially lodged in the narrow capillaries that surround liver tumors and selectively deliver a high dose of short-range beta radiation to the liver tumors. The physical properties of Y-90 resin microspheres facilitate even distribution of radioactivity within and around the liver metastases. SIRFLOX is an International, multi-center, open-label, randomized phase III study, which evaluated the efficacy and safety of combining modified FOLFOX6 (Oxaliplatin, 5-FU and Leucovorin) chemotherapy regimen with or without AVASTIN® (Bevacizumab) with SIRT, using Y-90 resin microspheres, as first line treatment in patients with unresectable liver only or liver dominant metastatic ColoRectal Cancer (mCRC). The randomization included 530 patients of whom 263 patients received mFOLFOX6 with or without AVASTIN® (Group A) and 267 patients received mFOLFOX6 + SIRT administered once with cycle 1, with or without AVASTIN® (Group B), with the treatment given until disease progression. Patients were stratified based on the extent of liver involvement (25% or less versus more than 25%), presence of extra hepatic disease (liver only versus liver dominant disease) and treatment with AVASTIN®, which was at the discretion of the attending physician. Forty percent of the patients had extra hepatic disease. The primary endpoint was Progression Free Survival (PFS). With a median follow up of 36.1 months, the median PFS in the liver was 12.6 months versus 20.5 months in Group A versus Group B respectively (HR=0.69; P=0.002). The hepatic Response Rate was 68.8% versus 78.7% (P=0.042), with a Complete Response Rate of 1.9% versus 6.0% (P=0.02) in Groups A and B respectively. Even though hematologic and gastrointestinal adverse events were higher in the SIRT group, the toxicity levels were acceptable. The authors concluded that the addition of SIRT to chemotherapy resulted in a 7.9 month improvement in Progression Free Survival in the liver, for patients with unresectable metastatic ColoRectal cancer (mCRC), with a 31% reduction in the risk of tumor progression in the liver. With the liver being the most common site of spread in patients with metastatic CRC, this study provides Level One evidence to support the use of SIRT in combination with chemotherapy in this patient group. SIRFLOX: Randomized phase III trial comparing first-line mFOLFOX6 ± bevacizumab (bev) versus mFOLFOX6 + selective internal radiation therapy (SIRT) ± bev in patients (pts) with metastatic colorectal cancer (mCRC). Gibbs P, Heinemann V, Sharma NK, et al. J Clin Oncol 33, 2015 (suppl; abstr 3502)</s
SIRFLOX is an International, multi-center, open-label, randomized phase III study, which evaluated the efficacy and safety of combining modified FOLFOX6 (Oxaliplatin, 5-FU and Leucovorin) chemotherapy regimen with or without AVASTIN® (Bevacizumab) with SIRT, using Y-90 resin microspheres, as first line treatment in patients with unresectable liver only or liver dominant metastatic ColoRectal Cancer (mCRC). The randomization included 530 patients of whom 263 patients received mFOLFOX6 with or without AVASTIN® (Group A) and 267 patients received mFOLFOX6 + SIRT administered once with cycle 1, with or without AVASTIN® (Group B), with the treatment given until disease progression. Patients were stratified based on the extent of liver involvement (25% or less versus more than 25%), presence of extra hepatic disease (liver only versus liver dominant disease) and treatment with AVASTIN®, which was at the discretion of the attending physician. Forty percent of the patients had extra hepatic disease. The primary endpoint was Progression Free Survival (PFS). With a median follow up of 36.1 months, the median PFS in the liver was 12.6 months versus 20.5 months in Group A versus Group B respectively (HR=0.69; P=0.002). The hepatic Response Rate was 68.8% versus 78.7% (P=0.042), with a Complete Response Rate of 1.9% versus 6.0% (P=0.02) in Groups A and B respectively. Even though hematologic and gastrointestinal adverse events were higher in the SIRT group, the toxicity levels were acceptable. The authors concluded that the addition of SIRT to chemotherapy resulted in a 7.9 month improvement in Progression Free Survival in the liver, for patients with unresectable metastatic ColoRectal cancer (mCRC), with a 31% reduction in the risk of tumor progression in the liver. With the liver being the most common site of spread in patients with metastatic CRC, this study provides Level One evidence to support the use of SIRT in combination with chemotherapy in this patient group. SIRFLOX: Randomized phase III trial comparing first-line mFOLFOX6 ± bevacizumab (bev) versus mFOLFOX6 + selective internal radiation therapy (SIRT) ± bev in patients (pts) with metastatic colorectal cancer (mCRC). Gibbs P, Heinemann V, Sharma NK, et al. J Clin Oncol 33, 2015 (suppl; abstr 3502)</s
Immediate ADT Confers Survival Benefit in Prostate Cancer Patients with “Biochemical Recurrence”
SUMMARY: Prostate cancer is the most common cancer in American men excluding skin cancer and 1 in 7 men will be diagnosed with prostate cancer during their lifetime. It is estimated that in the United States, about 220,800 new cases of prostate cancer will be diagnosed in 2015 and over 27,000 men will die of the disease. The major source of PSA (Prostate Specific Antigen) is the prostate gland and the PSA levels are therefore undetectable within 6 weeks after Radical Prostatectomy. Similarly, following Radiation Therapy, there is a gradual decline in PSA before reaching a post treatment nadir. A detectable PSA level after Radical Prostatectomy, or a rising PSA level following Radiation Therapy, is considered PSA failure or biochemical recurrence.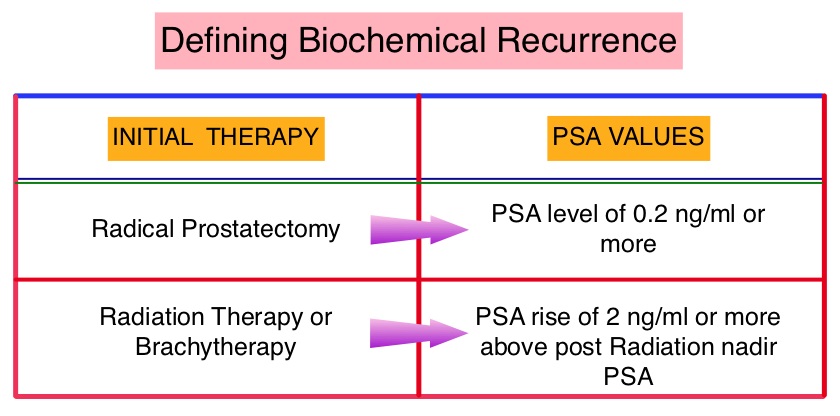 The American Urological Association suggested that a PSA of 0.2 ng/mL or higher after Radical Prostatectomy, defines PSA failure or relapse. A PSA rise of 2 ng/ml or more above post Radiation Therapy nadir is considered PSA failure or relapse. Approximately 35% of the patients with prostate cancer will experience PSA only relapse within 10 years of their primary treatment and a third of these patients will develop documented metastatic disease within 8 years following PSA only relapse. The development and progression of prostate cancer is driven by androgens. Androgen Deprivation Therapy (ADT) has therefore been the cornerstone of treatment of advanced prostate cancer and is the first treatment intervention for hormone sensitive prostate cancer. The appropriate time (immediate versus delayed) to start Androgen Deprivation Therapy (ADT) in patients with prostate cancer with rising Prostate-Specific Antigen (PSA), as the only sign of relapse, has remained unclear. This has been partly due to lack of patient accruals and patient reluctance to be randomized, in these clinical trials.
The American Urological Association suggested that a PSA of 0.2 ng/mL or higher after Radical Prostatectomy, defines PSA failure or relapse. A PSA rise of 2 ng/ml or more above post Radiation Therapy nadir is considered PSA failure or relapse. Approximately 35% of the patients with prostate cancer will experience PSA only relapse within 10 years of their primary treatment and a third of these patients will develop documented metastatic disease within 8 years following PSA only relapse. The development and progression of prostate cancer is driven by androgens. Androgen Deprivation Therapy (ADT) has therefore been the cornerstone of treatment of advanced prostate cancer and is the first treatment intervention for hormone sensitive prostate cancer. The appropriate time (immediate versus delayed) to start Androgen Deprivation Therapy (ADT) in patients with prostate cancer with rising Prostate-Specific Antigen (PSA), as the only sign of relapse, has remained unclear. This has been partly due to lack of patient accruals and patient reluctance to be randomized, in these clinical trials.
The authors conducted this randomized, prospective, phase III trial, to determine if immediate intervention with Androgen Deprivation Therapy (ADT) would improve Overall Survival (OS), compared with delayed ADT, in prostate cancer patients with PSA relapse, following definitive therapy, or in asymptomatic men not suitable for definitive therapy at the time of diagnosis. This analysis combined prostate cancer patients with PSA relapse enrolled in two separate studies. Two hundred and ninety three (N=293) eligible patients were randomly assigned 1:1 to immediate Androgen Deprivation Therapy (N= 142) or delayed ADT (N=151). The primary endpoint was unadjusted Overall Survival. Secondary endpoints included cancer-specific survival and time to clinical progression. The median follow up was 5 years. There was a statistically significant improvement in the Overall Survival, with a 45% reduction in the risk for death, for those receiving immediate ADT compared with the delayed treatment group (HR=0.55; P=0.05). Further, with immediate ADT, there was a statistically significant delay in the time to first local progression (HR= 0.51; P=0.001) as well as time to first metastatic disease (HR=0.54; P=0.018). The authors concluded that immediate Androgen Deprivation Therapy significantly improved Overall Survival and time to clinical progression for prostate cancer patients with PSA relapse, after definitive therapy. This benefit however must be weighed against the risks associated with long term Androgen Deprivation Therapy. TROG 03.06 and VCOG PR 01-03: The “Timing Of Androgen Deprivation therapy in prostate cancer patients with a rising PSA (TOAD)” collaborative randomised phase III trial. Duchesne GM, Bassett J, D’Este C, et al. J Clin Oncol 33, 2015 (suppl; abstr 5007)
Late Breaking Abstract – ASCO 2015 IMBRUVICA® in Combination with BR Regimen Shows Significant Benefit in Relapsed CLL patients
SUMMARY: The American Cancer Society estimates that approximately 14,620 new cases of Chronic Lymphocytic Leukemia (CLL) will be diagnosed in 2015 and approximately 4650 patients will die from the disease. CLL is a disease of the elderly and the average age at the time of diagnosis is 72 years. There are two main types of lymphocytes, B and T lymphocytes/cells. B-cell CLL is the most common type of leukemia in adults. Normal B-cell activation and proliferation is dependent on B-cell receptor (BCR) signaling. This signaling is also important for initiation and progression of B-cell lymphoproliferative disorders. Bruton’s Tyrosine Kinase (BTK) is a member of the Tec family of kinases, downstream of the B-cell receptor and is predominantly expressed in B-cells. It is a mediator of B-cell receptor signaling in normal and transformed B-cells. Following binding of antigen to the B-Cell Receptor, kinases such as Syk (Spleen Tyrosine Kinase), Lyn (member of the Src family of protein tyrosine kinases) and BTK (Bruton’s Tyrosine Kinase) are activated, with subsequent propagation through PI3K/Akt, MAPK, and NF-κB pathways. This results in B-cell activation and proliferation. IMBRUVICA® (Ibrutinib) is an oral, irreversible inhibitor of BTK and inhibits cell proliferation and promotes programmed cell death (Apoptosis) by blocking B-cell activation and signaling. The FDA initially granted accelerated approval to IMBRUVICA® in February 2014 for previously treated patients with CLL and this was followed by full FDA approval and a new treatment indication for high-risk CLL patients with 17p deletions, in July 2014. Previously published studies had shown significant Response Rates and and Event-Free Survival with BR (Bendamustine-TREANDA® and Rituximab-RITUXAN®) in FLUDARA® (Fludarabine) refractory patients, with Chronic Lymphocytic Leukemia.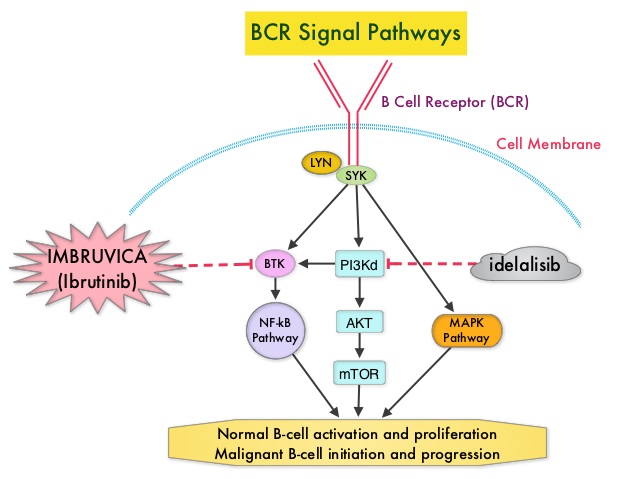
The HELIOS study is a double-blind, randomized, phase III trial which evaluated the benefit of combining IMBRUVICA® with BR compared to placebo plus BR, in patients with previously treated, relapsed/refractory Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma. In this study, of the 578 randomized patients, 289 patients received a maximum of six cycles of BR with IMBRUVICA® 420 mg PO daily and 289 patients received BR with placebo. The median patient age was 64 years, patients had received a median of two prior therapies and 38% of the patients had Rai Stage III/IV disease. Patients with 17p deletions in more than >20% of cells, were excluded. The planned six cycles of BR were completed by 83% in the IMBRUVICA® group and 78% in the placebo group. The primary endpoint was Progression Free Survival (PFS). Secondary endpoints included Overall Survival (OS) and Overall Response Rate (ORR). Following an interim analysis, this study was unblinded as there was a significant PFS benefit with IMBRUVICA® and patients receiving placebo, were allowed to cross over to the IMBRUVICA® group, per study protocol,. Thirty one percent (31%) of the patients in the BR plus placebo group with confirmed progressive disease crossed over to receive BR plus IMBRUVICA®. At a median follow up of 17.2 months, the PFS in the IMBRUVICA® plus BR group was not yet reached whereas the PFS was 13.3 months for patients receiving placebo plus BR (HR=0.203; P<0.0001). This PFS benefit was seen across subgroups of high-risk patients as well. The ORR was 82.7% in the IMBRUVICA® plus BR group compared to 67.8% in the placebo plus BR group (P <0.0001). Complete Response (CR) rates which included CR with incomplete blood count recovery were 10.4% versus 2.8% with IMBRUVICA® and placebo, respectively. The median OS was not reached. The incidence of most adverse events were comparable between the two treatment groups and the most frequent side effects were neutropenia affecting about 55% of the patients and nausea experienced by about 35% of the patients. The authors concluded that IMBRUVICA® plus BR resulted in an 80% reduction in the risk of disease progression, as well as improved Overall Response Rates, compared to placebo plus BR. This triplet combination of IMBRUVICA®, TREANDA® and RITUXAN® should therefore be considered an important treatment option for patients with previously treated Chronic Lymphocytic Leukemia and Small Lymphocytic Lymphoma. Ibrutinib combined with bendamustine and rituximab (BR) in previously treated chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL): first results from a randomized, double-blind, placebo-controlled, phase III study. Chanan-Khan AAA, Cramer P, Demirkan F, et al. J Clin Oncol. 2015;33 (suppl; abstr LBA7005).
Daily Aspirin May Improve Survival after Diagnosis of Colorectal Cancer
SUMMARY:The American Cancer Society estimates that approximately 133,000 new cases of ColoRectal Cancer (CRC) will be diagnosed in the United States in 2015 and close to 50,000 are expected to die of the disease. Several epidemiological studies as well as randomized controlled trials have shown that Aspirin reduces the incidence of ColoRectal Cancer (CRC) and CRC associated mortality. Platelets have long been implicated in the mechanism of tumor metastases. More recent data suggests that platelets may play a role in tumorigenesis as well, through the release of angiogenic and growth factors due to overexpression of COX-2. Daily low dose Aspirin inhibits COX-1 and COX-2. 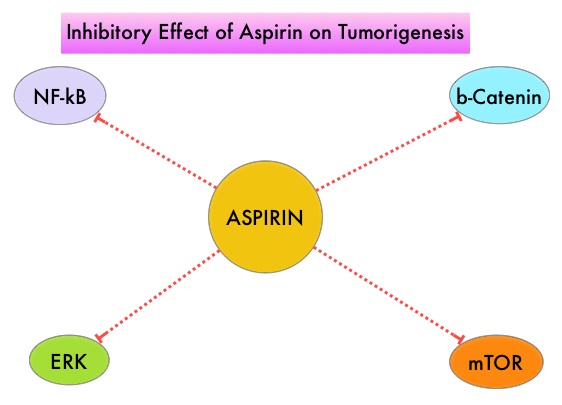 It is postulated that Aspirin also works by COX-independent mechanisms such as, the inhibition of NF-kB and Wnt/ β-catenin signaling, which may play a role in its chemopreventive properties. Even though the benefits of Aspirin in the primary prevention of CRC remains well established, the role of Aspirin in secondary prevention in patients with CRC is unclear. The authors conducted this trial to evaluate the association between Aspirin use after diagnosis of CRC with CRC-Specific Survival (CSS) and Overall Survival (OS) in the largest group of patients ever studied. The study authors in this retrospective study identified 25,644 patients in the Cancer Registry of Norway, diagnosed with ColoRectal Cancer (CRC) from 2004 through 2011. Using the Norwegian Prescription Database, the authors were then able to establish that 6,109 patients in this large cohort had documented exposure to Aspirin. Exposure to Aspirin was defined as a prescription for more than 6 months of Aspirin following a diagnosis of CRC. The median follow up was 2.2 years. The authors performed a multivariate regression analysis controlling for age, gender, tumor stage, tumor differentiation and noted that exposure to Aspirin post-diagnosis, independently improved ColoRectal Cancer (CRC) -Specific Survival (HR=0.75; P<0.001) and Overall Survival (HR=0.86; P<0.001). The authors concluded that in this large group of unselected ColoRectal Cancer (CRC) patients, exposure to Aspirin after the diagnosis of CRC is independently associated with improved Colorectal Cancer-Specific Survival and Overall Survival. They added that because of the risk of bleeding, the risk–benefit should be assessed before Aspirin is routinely recommended to this patient population. Impact of aspirin as secondary prevention in an unselected cohort of 25,644 patients with colorectal cancer: A population-based study. Bains S, Mahic M, Cvancarova M, et al. J Clin Oncol 33, 2015 (suppl; abstr 3504)
It is postulated that Aspirin also works by COX-independent mechanisms such as, the inhibition of NF-kB and Wnt/ β-catenin signaling, which may play a role in its chemopreventive properties. Even though the benefits of Aspirin in the primary prevention of CRC remains well established, the role of Aspirin in secondary prevention in patients with CRC is unclear. The authors conducted this trial to evaluate the association between Aspirin use after diagnosis of CRC with CRC-Specific Survival (CSS) and Overall Survival (OS) in the largest group of patients ever studied. The study authors in this retrospective study identified 25,644 patients in the Cancer Registry of Norway, diagnosed with ColoRectal Cancer (CRC) from 2004 through 2011. Using the Norwegian Prescription Database, the authors were then able to establish that 6,109 patients in this large cohort had documented exposure to Aspirin. Exposure to Aspirin was defined as a prescription for more than 6 months of Aspirin following a diagnosis of CRC. The median follow up was 2.2 years. The authors performed a multivariate regression analysis controlling for age, gender, tumor stage, tumor differentiation and noted that exposure to Aspirin post-diagnosis, independently improved ColoRectal Cancer (CRC) -Specific Survival (HR=0.75; P<0.001) and Overall Survival (HR=0.86; P<0.001). The authors concluded that in this large group of unselected ColoRectal Cancer (CRC) patients, exposure to Aspirin after the diagnosis of CRC is independently associated with improved Colorectal Cancer-Specific Survival and Overall Survival. They added that because of the risk of bleeding, the risk–benefit should be assessed before Aspirin is routinely recommended to this patient population. Impact of aspirin as secondary prevention in an unselected cohort of 25,644 patients with colorectal cancer: A population-based study. Bains S, Mahic M, Cvancarova M, et al. J Clin Oncol 33, 2015 (suppl; abstr 3504)
Late Breaking Abstract – ASCO 2015 ARIMIDEX® may be a Better Treatment Option Compared to Tamoxifen in Postmenopausal Women with DCIS
SUMMARY: Breast cancer is the most common cancer among women in the US and about 1 in 8 women (12%) will develop invasive breast cancer during their lifetime. Approximately, 231,840 new cases of invasive breast cancer will be diagnosed in 2015 and over 40,000 women will die of the disease.Estrogen Receptor (ER) positive breast cancer cells are driven by estrogens. Tamoxifen is a nonsteroidal Selective Estrogen Receptor Modulator (SERM) and works mainly by binding to the Estrogen Receptor and thus blocks the proliferative actions of estrogen on the mammary tissue. Anastrozole is a non-steroidal Aromatase Inhibitor that binds reversibly to the aromatase enzyme and inhibits the conversion of androgens to estrogens in the extra-gonadal tissues. Aromatase Inhibitors such as ARIMIDEX® have been proven to be superior to Tamoxifen, as adjuvant therapy, in postmenopausal patients with hormone receptor positive breast cancer. It was however not known whether ARIMIDEX® was superior to Tamoxifen in preventing the recurrence of breast cancer.
NSABP B-35 is a randomized phase III trial which compared ARIMIDEX® to Tamoxifen, in preventing the recurrence of breast cancer, in postmenopausal women with Ductal Carcinoma In Situ (DCIS), who underwent lumpectomy and radiation therapy. Of the 3,104 patients who were enrolled and randomized, 1552 patients received ARIMIDEX® 1 mg PO daily and 1552 patients received Tamoxifen 20 mg PO daily. Treatment was continued for 5 years. Enrolled patients had tumors with no invasive component, Estrogen or Progesterone Receptors were positive and margins of resection were clear. The primary endpoint was Breast Cancer-Free Interval (BCFI), defined as the time from randomization to any breast cancer event including local, regional, or distant recurrence or contralateral invasive cancer or DCIS. With a median follow up of 8.6 years, the 10 year Breast Cancer–Free Interval rates were 93.5% with ARIMIDEX® versus 89.2% with Tamoxifen, and this was statistically significant (HR=0.73, P=0.03). This benefit was more so in women less than 60 years of age, with a Breast Cancer–Free Interval rates of 94.9% with ARIMIDEX® and 88.2% with Tamoxifen (HR=0.52, P=0.003). However, in women over 60 years of age, there were no significant differences in outcomes noted between the ARIMIDEX® and Tamoxifen groups. The incidence of invasive contralateral breast cancer was reduced by 45% (HR=0.55, P=0.03) in the ARIMIDEX® group, compared to Tamoxifen group. Adverse events were less common with ARIMIDEX® compared to Tamoxifen. The authors concluded that for postmenopausal women with DCIS treated with lumpectomy and radiation, the 10 year Breast Cancer–Free Interval rates are significantly higher with 5 years of ARIMIDEX® than Tamoxifen and ARIMIDEX® may also be a consideration for those women, who are concerned about the risk of thromboembolic events and uterine cancer with Tamoxifen treatment. Primary results, NRG Oncology/NSABP B-35: A clinical trial of anastrozole (A) versus tamoxifen (tam) in postmenopausal patients with DCIS undergoing lumpectomy plus radiotherapy. Margolese RG, Cecchini RS, Julian TB, et al. J Clin Oncol 33, 2015 (suppl; abstr LBA500)
Late Breaking Abstract – ASCO 2015 Adjuvant Whole Brain Radiation Therapy Not Recommended After Stereotactic RadioSurgery
SUMMARY: Brain metastases from an extracranial primary, occur in approximately 15% of cancer patients and this is estimated to be about 400,000 to 600,000 patients annually. The incidence of brain metastases has been on the rise with the availability of more effective systemic therapies and better control of systemic disease. The most frequent malignancies associated with brain metastases include Lung cancer, Breast cancer and Melanoma. Majority of the patients with brain metastases have synchronous extracerebral metastases. A significant number of patients present with solitary or fewer than 3 brain metastases and they may be amenable to focal therapeutic interventions. However, Whole Brain Radiation Therapy (WBRT) has been the standard treatment strategy since the 1950’s. It is also well recognized that WBRT can be associated with neurocognitive dysfunction. Stereotactic RadioSurgery (SRS) is a non-surgical procedure that allows delivery of significantly higher doses of precisely focused radiation to the tumor, compared to conventional radiation therapy, with less collateral damage to the surrounding normal tissue. The technologies used for SRS include GAMMA KNIFE® which uses highly focused gamma rays, Proton Beam therapy which uses ionized hydrogen or Protons, Linear Accelerator and CYBER KNIFE® which use Photons, to target the tumor tissue.
NCCTG N0574 is a federally funded, randomized phase III clinical trial, designed to determine whether cognitive deterioration occurred less frequently with SRS alone compared to SRS followed by WBRT, in patients with 1-3 brain metastases. In this study, 213 patients with 1-3 brain metastases, each measuring less than 3 cm by contrast MRI, were enrolled and randomized to SRS alone or SRS plus WBRT. All patients underwent cognitive testing before and after treatment. Sixty eight percent (68%) of the enrolled patients had a Lung primary and the median age was 60 years. Baseline characteristics were similar in both treatment groups. The median follow up was 7.2 months. The authors used several tools to assess cognitive dysfunction and the primary endpoint was the cognitive decline at 3 months following treatment. It was noted that at 3 months, with the addition of WBRT to SRS, 91.7% of patients experienced cognitive decline compared with 63.5% for those receiving SRS alone (P=0.0007) and there was statistically significant decline in immediate recall, delayed recall and verbal fluency, in the SRS plus WBRT group. Patients who received SRS plus WBRT also reported significantly worse Quality of Life. There was however better intracranial tumor control at 6 and 12 months with SRS plus WBRT compared to SRS alone (P< 0.001), but this local control had no significant impact on the median Overall Survival (OS), with similar OS outcomes noted in both treatment groups (P=0.93). The authors concluded that the addition of WBRT to SRS can result in significant decline in neurocognitive function, without any Overall Survival benefit, compared to SRS alone. It is therefore recommended that patients with newly diagnosed brain metastases amenable to SRS, be closely monitored after SRS, with consideration given to WBRT, at the time of symptomatic progression. NCCTG N0574 (Alliance): A phase III randomized trial of whole brain radiation therapy (WBRT) in addition to radiosurgery (SRS) in patients with 1 to 3 brain metastases. Brown PD, Asher AL, Ballman KV, et al. J Clin Oncol 33, 2015 (suppl; abstr LBA4)
Late Breaking Abstract – ASCO 2015 OPDIVO® Improves Overall Survival in Non- Squamous NSCLC Patients
SUMMARY: Lung cancer is the second most common cancer in both men and women and accounts for about 13% of all new cancers and 27% of all cancer deaths. It is the leading cause of cancer death among both men and women. The American Cancer Society estimates that over 221,200 new cases of lung cancer will be diagnosed in the United States in 2015 and over 158,000 patients will die of the disease. Non Small Cell Lung Cancer (NSCLC) accounts for approximately 85% of all lung cancers. Of the three main subtypes of Non Small Cell Lung Cancer (NSCLC), 25% are Squamous cell carcinomas, 40% are Adenocarcinomas and 10% are Large cell carcinomas. The treatment paradigm for solid tumors has been rapidly evolving with a better understanding of the Immune checkpoints. Immune checkpoints are cell surface inhibitory proteins/receptors that are expressed on activated T cells. They harness the immune system and prevent uncontrolled immune reactions. Survival of cancer cells in the human body may be to a significant extent, related to their ability to escape immune surveillance, by inhibiting T lymphocyte activation. The T cells of the immune system therefore play a very important role in modulating the immune system.  Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4), also known as CD152, PD-1(Programmed cell Death-1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. The first Immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® (Ipilimumab) , an antibody that blocks Immune checkpoint protein/receptor CTLA- 4, has been shown to prolong overall survival in patients with previously treated, unresectable or metastatic melanoma. OPDIVO® (Nivolumab) is a fully human, immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the T cells. The U. S. Food and Drug Administration granted approval to OPDIVO®, for the treatment of patients with metastatic Squamous Non-Small Cell Lung Cancer (NSCLC), with progression on or after platinum based chemotherapy. CheckMate 057 is a randomized, international, phase 3 study designed to evaluate the benefit of OPDIVO® for patients with Non-Squamous (NSQ) NSCLC who had progressed after platinum-based doublet chemotherapy. A total of 582 patients were randomized to receive OPDIVO® 3 mg/kg IV every 2 weeks (n=292) or TAXOTERE® 75 mg/m2 IV every 3 weeks (n=290). Eligible patients included those with advanced Non-Squamous NSCLC who had progressed after platinum-based doublet chemotherapy and a Tyrosine Kinase Inhibitor (TKI), if deemed eligible for a TKI. Treatment was continued until disease progression or unacceptable toxicity. The primary clinical endpoint was Overall Survival (OS). Secondary endpoints included Objective Response Rate (ORR), Progression Free Survival (PFS), Efficacy based on PD-L1 expression, Quality of Life, and Safety. The study was stopped earlier than expected following assessment by the independent Data Monitoring Committee (DMC) which concluded that the study met its endpoint, demonstrating superior overall survival, in patients receiving OPDIVO®, compared to the control group. Patients in the OPDIVO®, group had a significantly higher median OS compared to those in the TAXOTERE® group (12.2 months versus 9.4 months, Hazard Ratio [HR] 0.73, P=0.0015). This meant a 27% reduction in the risk of death in the OPDIVO® group and this survival benefit was seen in all predefined subgroup of patients. The Objective Response Rate (ORR) was also significantly higher for patients receiving OPDIVO® compared to TAXOTERE® (19% versus 12%, P=0.0246) and the median duration of response (DOR) was significantly higher for the OPDIVO® group (17.2 months) vs the TAXOTERE® group (5.6 months). More importantly, when tumor PD-L1 expression was correlated with Overall Survival, the median OS for OPDIVO® was 17.2 months, 18.2 months, and 19.4 months for patients with tumors having 1% or higher, 5% or higher, and 10% or higher of cells staining positive for PD-L1, respectively, compared with 9.0 months, 8.1 months, and 8.0 months with TAXOTERE® treatment. Even though this study showed significant survival outcomes for patients expressing any level of PD-L1, the magnitude of benefit was even more so, in patients with tumors expressing higher levels of PD-L1. PD-L1 expression may therefore be a predictor of response, although this should not yet be used for patient selection. Grade 3-5 adverse events occurred more often in the TAXOTERE® group compared to the OPDIVO® group (54% vs 10%). Based on this compelling data, the authors concluded that OPDIVO® significantly improves Overall Survival when compared to TAXOTERE®, in patients with advanced non-Squamous NSCLC, after failure of platinum based doublet therapy. Phase III, randomized trial (CheckMate 057) of nivolumab (NIVO) versus docetaxel (DOC) in advanced non-squamous cell (non-SQ) non-small cell lung cancer (NSCLC). Paz-Ares L, Horn L, Borghaei H, et al. J Clin Oncol 33, 2015 (suppl; abstr LBA109)</s
Under normal circumstances, inhibition of an intense immune response and switching off the T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. With the recognition of Immune checkpoint proteins and their role in suppressing antitumor immunity, antibodies are being developed that target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4 (Cytotoxic T-Lymphocyte Antigen 4), also known as CD152, PD-1(Programmed cell Death-1), etc. By doing so, one would expect to unleash the T cells, resulting in T cell proliferation, activation and a therapeutic response. The first Immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® (Ipilimumab) , an antibody that blocks Immune checkpoint protein/receptor CTLA- 4, has been shown to prolong overall survival in patients with previously treated, unresectable or metastatic melanoma. OPDIVO® (Nivolumab) is a fully human, immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2, thereby undoing PD-1 pathway-mediated inhibition of the immune response and unleashing the T cells. The U. S. Food and Drug Administration granted approval to OPDIVO®, for the treatment of patients with metastatic Squamous Non-Small Cell Lung Cancer (NSCLC), with progression on or after platinum based chemotherapy. CheckMate 057 is a randomized, international, phase 3 study designed to evaluate the benefit of OPDIVO® for patients with Non-Squamous (NSQ) NSCLC who had progressed after platinum-based doublet chemotherapy. A total of 582 patients were randomized to receive OPDIVO® 3 mg/kg IV every 2 weeks (n=292) or TAXOTERE® 75 mg/m2 IV every 3 weeks (n=290). Eligible patients included those with advanced Non-Squamous NSCLC who had progressed after platinum-based doublet chemotherapy and a Tyrosine Kinase Inhibitor (TKI), if deemed eligible for a TKI. Treatment was continued until disease progression or unacceptable toxicity. The primary clinical endpoint was Overall Survival (OS). Secondary endpoints included Objective Response Rate (ORR), Progression Free Survival (PFS), Efficacy based on PD-L1 expression, Quality of Life, and Safety. The study was stopped earlier than expected following assessment by the independent Data Monitoring Committee (DMC) which concluded that the study met its endpoint, demonstrating superior overall survival, in patients receiving OPDIVO®, compared to the control group. Patients in the OPDIVO®, group had a significantly higher median OS compared to those in the TAXOTERE® group (12.2 months versus 9.4 months, Hazard Ratio [HR] 0.73, P=0.0015). This meant a 27% reduction in the risk of death in the OPDIVO® group and this survival benefit was seen in all predefined subgroup of patients. The Objective Response Rate (ORR) was also significantly higher for patients receiving OPDIVO® compared to TAXOTERE® (19% versus 12%, P=0.0246) and the median duration of response (DOR) was significantly higher for the OPDIVO® group (17.2 months) vs the TAXOTERE® group (5.6 months). More importantly, when tumor PD-L1 expression was correlated with Overall Survival, the median OS for OPDIVO® was 17.2 months, 18.2 months, and 19.4 months for patients with tumors having 1% or higher, 5% or higher, and 10% or higher of cells staining positive for PD-L1, respectively, compared with 9.0 months, 8.1 months, and 8.0 months with TAXOTERE® treatment. Even though this study showed significant survival outcomes for patients expressing any level of PD-L1, the magnitude of benefit was even more so, in patients with tumors expressing higher levels of PD-L1. PD-L1 expression may therefore be a predictor of response, although this should not yet be used for patient selection. Grade 3-5 adverse events occurred more often in the TAXOTERE® group compared to the OPDIVO® group (54% vs 10%). Based on this compelling data, the authors concluded that OPDIVO® significantly improves Overall Survival when compared to TAXOTERE®, in patients with advanced non-Squamous NSCLC, after failure of platinum based doublet therapy. Phase III, randomized trial (CheckMate 057) of nivolumab (NIVO) versus docetaxel (DOC) in advanced non-squamous cell (non-SQ) non-small cell lung cancer (NSCLC). Paz-Ares L, Horn L, Borghaei H, et al. J Clin Oncol 33, 2015 (suppl; abstr LBA109)</s