SUMMARY: The American Cancer Society estimates that 63,340 new cases of kidney cancer will be diagnosed in the United States in 2018 and about 14,970 people will die from the disease. Renal Cell Carcinoma (RCC) is by far the most common type of kidney cancer and is about twice as common in men as in women. Modifiable risk factors include smoking, obesity, workplace exposure to certain substances and high blood pressure. The five year survival of patients with advanced RCC is less than 10% and there is significant unmet need for improved therapies for this disease. SUTENT® (Sunitinib) is a MultiKinase Inhibitor (MKI) which simultaneously targets the tumor cell wall, vascular endothelial cell wall as well as the pericyte/fibroblast/vascular/ smooth vessel cell wall and is capable of specifically binding to tyrosine kinases, inhibiting the earlier signaling events and thereby inhibits phosphorylation of VEGF receptor, PDGF receptor, FLT-3 and c-KIT. SUTENT® is the standard first-line intervention for treatment naïve patients with advanced RCC. In a large, multi-center, randomized, phase III study, the median Progression Free Survival (PFS) with SUTENT® was 9.5 months, the Objective Response Rate (ORR) was 25%, and the median Overall Survival was 29.3 months, when compared with Interferon Alfa, in patients with treatment-naïve Renal Cell Carcinoma. This was however associated with a high rate of hematological toxicities.
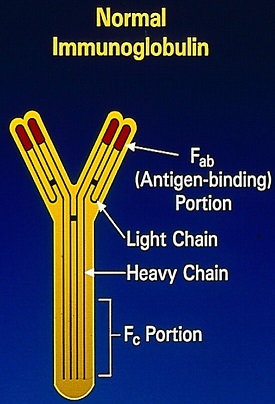
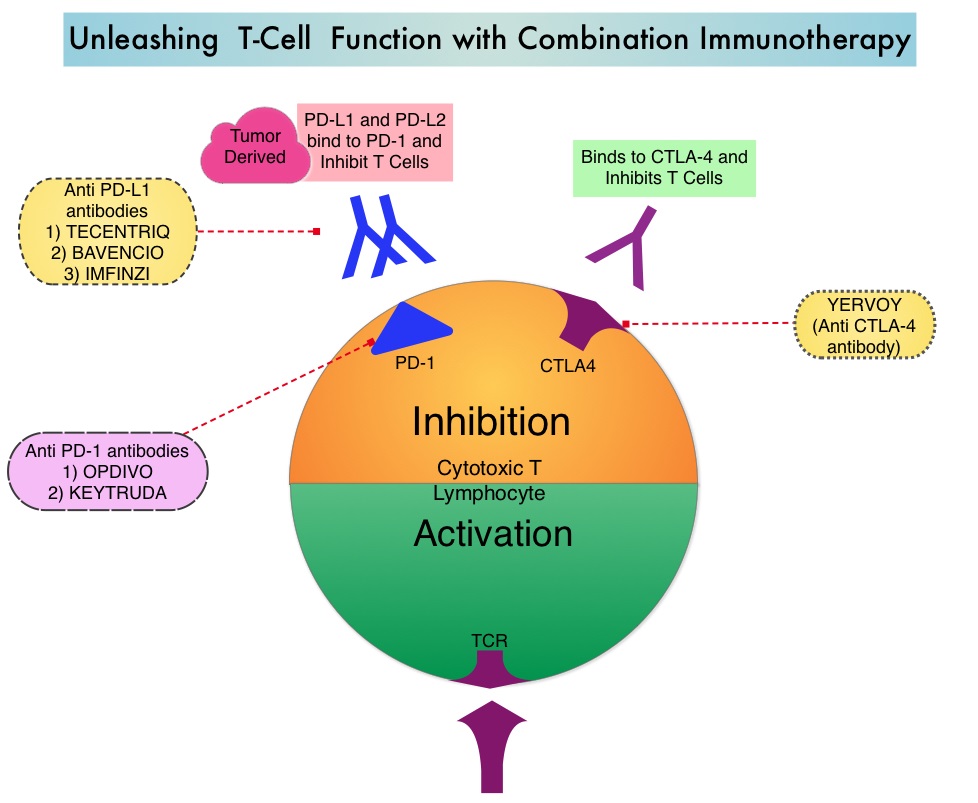
KEYTRUDA® (Pembrolizumab) is a fully humanized, Immunoglobulin G4, anti-PD-1, monoclonal antibody, that binds to the PD-1 receptor and blocks its interaction with ligands PD-L1 and PD-L2. It thereby reverses the PD-1 pathway-mediated inhibition of the immune response and unleashes the tumor-specific effector T cells. INLYTA® (Axitinib) is a kinase inhibitor and inhibits Receptor Tyrosine Kinases including Vascular Endothelial Growth Factor Receptors (VEGFR)-1, VEGFR-2, and VEGFR-3 at therapeutic plasma concentrations. These receptors have been implicated in pathologic angiogenesis, tumor growth, and cancer progression. Previously published data from a Phase I clinical trial showed that antitumor activity with a combination of KEYTRUDA® and INLYTA® was superior to monotherapy with either PD-1/PD-L1 inhibitor or INLYTA®, in treatment-naïve patients with advanced RCC. Further unlike excess toxicities associated with a combination of VEGF and PD-1 checkpoint inhibitors, a combination of INLYTA® and PD-1 inhibitor was associated with fewer liver function test abnormalities and less fatigue. The excess toxicities have been attributed to off-target effects of multitargeted Tyrosine Kinase Inhibitors.
KEYNOTE-426 is a pivotal, open label, randomized, double-arm, Phase III trial in which the safety and efficacy of KEYTRUDA® in combination with INLYTA® as first-line treatment for advanced or metastatic, clear cell RCC, was compared to SUTENT®. In this study, 861 patients treatment naïve patients who had prior nephrectomy were randomly assigned to receive KEYTRUDA 200 mg IV every three weeks along with INLYTA® 5 mg orally twice daily for up to 24 months, or SUTENT® 50 mg orally once daily for four weeks followed by no treatment for two weeks, given continuously. The dual Primary endpoints were Overall Survival (OS) and Progression Free Survival (PFS). The Secondary endpoints included Objective Response Rate (ORR), Disease Control Rate (DCR), and Duration of Response (DOR). PFS and OS were assessed at 12, 18 and 24 months.
Merck, the manufacturer of KEYTRUDA® in a press release on October 18, 2018 announced that based on the first interim analysis by the independent Data Monitoring Committee (DMC), the study had met the coprimary endpoints and the combination of KEYTRUDA® and INLYTA® resulted in statistically significant and clinically meaningful improvements in Overall Survival and Progression Free Survival, compared to SUTENT® monotherapy. The study also met the key Secondary endpoint of Objective Response Rate, with significant improvements for the KEYTRUDA® and INLYTA® combination, compared with SUTENT® monotherapy. Results for OS, PFS and ORR were consistent regardless of PD-L1 expression and across all risk groups. It was noted that the safety profile of KEYTRUDA® and INLYTA® in this trial was generally consistent with that observed in previously reported studies for each therapy.
According to the manufacturer, this is the first time that combination treatment with an anti PD-1 inhibitor achieved the dual Primary endpoints of Overall Survival and Progression Free Survival, as first line therapy in advanced RCC. Merck’s KEYTRUDA® (pembrolizumab) in Combination with Pfizer’s Inlyta® (axitinib) Significantly Improved Overall Survival (OS) and Progression-free Survival (PFS) as First-Line Therapy for Advanced or Metastatic Renal Cell Carcinoma. Merck. Published October 18, 2018.