
SUMMARY: The American Cancer Society estimates that in 2019, there will be an estimated 1,762,450 new cancer cases diagnosed and 606,880 cancer deaths in the United States. Immunotherapy with Immune Checkpoint Inhibitors (ICIs) has revolutionized cancer care and has become one of the most effective treatment options by improving Overall Response Rate and prolongation of survival across multiple tumor types. These agents target Programmed cell death protein-1 (PD-1), Programmed cell death ligand-1 (PD-L1), Cytotoxic T-Lymphocyte-Associated protein-4 (CTLA-4), and many other important regulators of the immune system.
Preclinical studies have suggested that immune-based therapies for cancer may have a very complex interplay with the host’s microbiome and there may be a relationship between gut bacteria and immune response to cancer. The crosstalk between microbiota in the gut and the immune system allows for the tolerance of commensal bacteria (normal microflora) and oral food antigens and at the same time enables the immune system to recognize and attack opportunistic bacteria. Immune Checkpoint Inhibitors strongly rely on the influence of the host’s microbiome, and the gut microbial diversity enhances mucosal immunity, dendritic cell function, and antigen presentation. Broad-spectrum antibiotics can alter the bacterial composition and bacterial diversity of our gut, by killing the good bacteria. It has been postulated that this may negate the benefits of immunotherapy and influence treatment outcomes.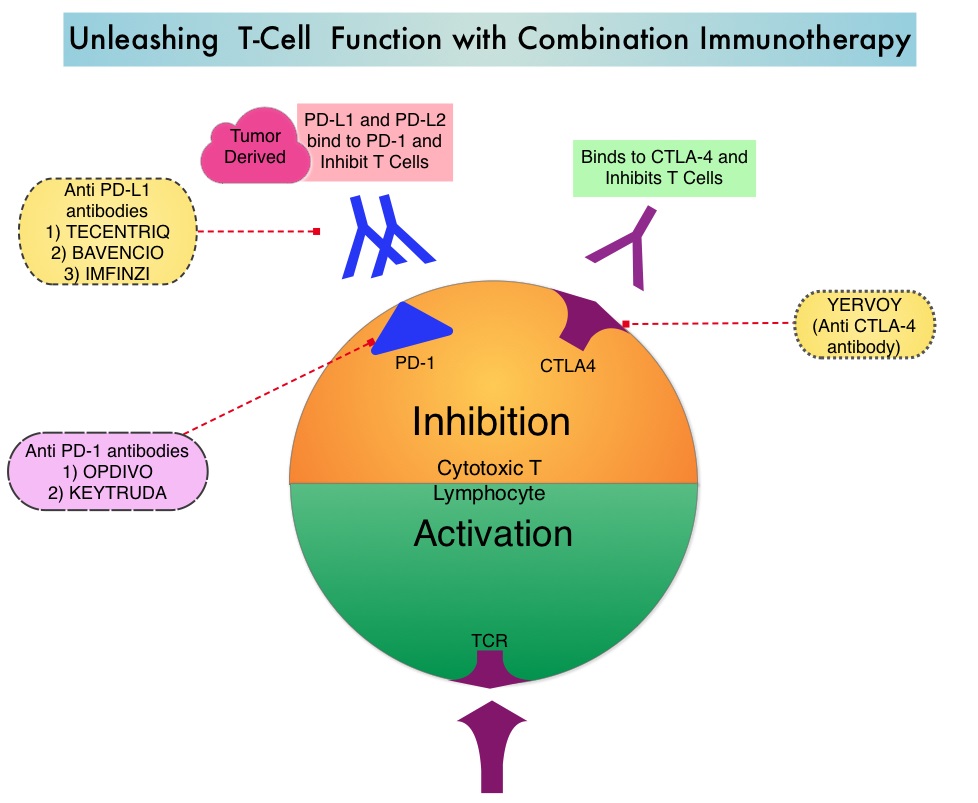
The authors conducted this study to determine whether there was an association between antibiotic therapy administered prior to or concurrently with ICI therapy and Overall Survival (OS) and Response Rates, in patients with cancer, treated with ICIs in routine clinical practice. In this prospective, multicenter cohort study, 196 patients with cancer who received ICI therapy were recruited at two tertiary care centers between January 2015 and April 2018. Majority of enrolled patients had Non-Small Cell Lung Cancer (N=119), but patients with Melanoma (N=38) as well as Urologic and Head and Neck cancers (N=39) were also included in the analysis. The median age was 68 years, and majority of patients had metastatic disease at the time of treatment initiation with ICIs and 96% of patients received anti-PD-1/PD-L1 therapy alone. Broad spectrum antibiotics up to 30 days prior to commencement of ICI qualified as prior antibiotic exposure whereas concurrent treatment with antibiotics was defined as antibiotic treatment from the first day of ICI treatment until cessation. Beta-lactams were the most commonly prescribed antibiotic class, and were given as a single course for less than 7 days. When antibiotics were administered concurrently with ICIs, patients tended to be treated longer and with multiple courses. The common indication for both prior and concurrent antibiotic treatment was respiratory infections, and 15% of patients received antibiotic therapy prior to ICI therapy, whereas 35% of patients received antibiotics concurrently with ICIs. The Primary endpoint was Overall Survival (OS), calculated from the time of ICI therapy commencement and radiologic response to treatment, with disease refractory to ICI therapy defined as progressive disease 6-8 weeks after the first ICI dose, without evidence of pseudoprogression.
In this analysis, antibiotic treatment prior to ICI therapy had a significant adverse effect on Overall Survival, with a median survival of only 2 months for those who received prior antibiotic treatment versus 26 months for antibiotic-naive patients (HR=7.4; P<0.001). Further, patients who had received prior antibiotic treatment had a higher likelihood of primary refractoriness to ICIs, compared to those who did not receive antibiotics (81% versus 44% (P<0.001). The poor OS outcomes when patients received antibiotic treatment prior to ICI therapy were noted, irrespective of tumor site (OS in NSCLC 26 vs 2.5 months, P<0.001, OS in Melanoma 14 vs 3.9 months, P<0.001, OS in other tumors 11 vs 1.1 months, P <0.001). Multivariate analyses confirmed that prior antibiotic therapy and response to ICI therapy were associated with OS, independent of tumor site, disease burden, and performance status. Antibiotic treatment administered concurrently with ICIs however, was not associated with worse Overall Survival.
It was concluded that treatment with antibiotics prior to therapy with Immune Checkpoint Inhibitors in routine clinical practice, is associated with a worse treatment response and Overall Survival in unselected group of patients. This study suggests that timing of antibiotic exposure may be crucial and the authors recommend that studies are urgently required to investigate antibiotic-mediated alterations of gut microbiota as a determinant of poorer outcomes, following treatment with Immune Checkpoint Inhibitors. Association of Prior Antibiotic Treatment With Survival and Response to Immune Checkpoint Inhibitor Therapy in Patients With Cancer. Pinato DJ, Howlett S, Ottaviani D, et al. JAMA Oncol. 2019, Sep 12. doi: 10.1001/jamaoncol.2019.2785. [Epub ahead of print]
