
SUMMARY: The FDA has granted Breakthrough Therapy Designation to immunotherapy with CTL019, which are genetically engineered T-cells. Chimeric Antigen Receptor (CAR) T-cell therapy is a type of immunotherapy in which T cells collected from the patient’s own blood and are genetically engineered to produce special receptors on their surface called chimeric antigen receptors (CAR’s). The cytotoxic T cells with these chimeric antigen receptors on their surface are now able to recognize a specific antigen on tumor cells. These engineered CAR T-cells which are grown in the lab are then infused into the patient and they in turn proliferate in the patient’s body and the engineered receptor on their surface help recognize and kill cancer cells that expresses that specific antigen. CTL019 are genetically engineered T-cells using CAR technology that seeks out cancer cells expressing the antigen CD19, which is found uniquely on B cells and destroy them.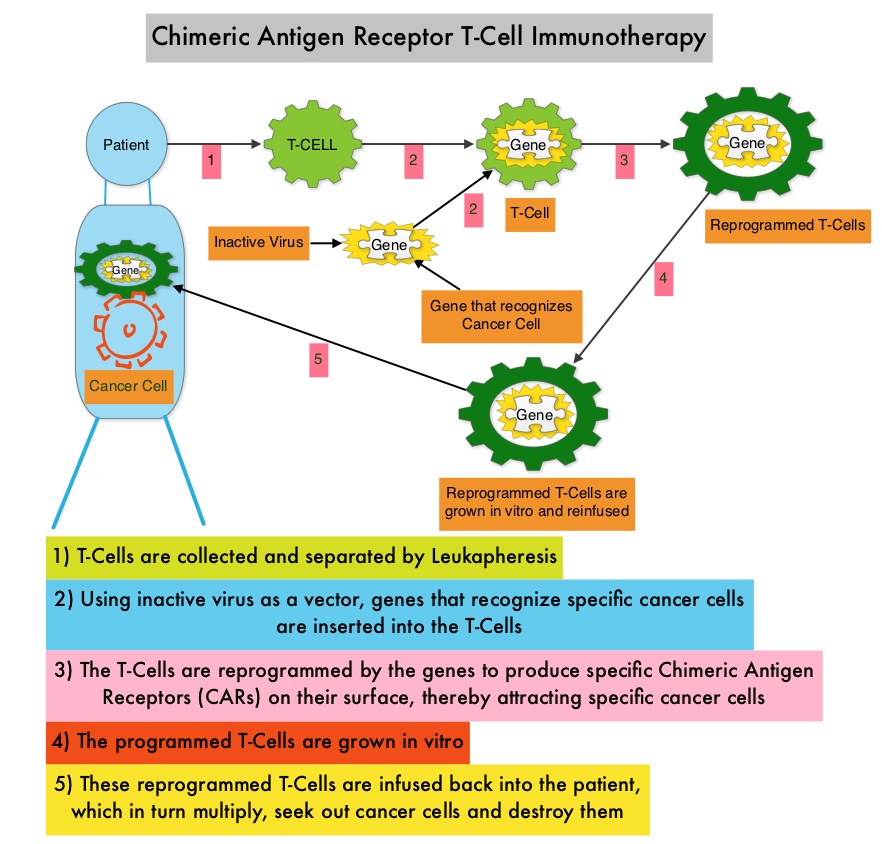 Patients, following treatment with CAR T-cells, develop B-cell aplasia (absence of CD19 positive cells) due to B-cell destruction and may need immunoglobin replacement. Hence, B-cell aplasia can be a useful therapeutic marker, as continued B-cell aplasia has been seen in all patients who had sustained remission, following CAR T-cell therapy. Cytokine Release Syndrome, an inflammatory process is the most common and serious side effect of CAR T-cell therapy and is associated with marked elevation of Interleukin-6. Cytokine release is important for T-cell activation and can result in high fevers and myalgias. This is usually self limiting although if severe can be associated with hypotension and respiratory insufficiency. Tocilizumab, an Interleukin-6 receptor blocking antibody produces a rapid improvement in symptoms. This is however not recommended unless the symptoms are severe and life threatening, as blunting the cytokine response can in turn negate T-cell proliferation. Elevated serum Ferritin and C-reactive protein levels are surrogate markers for severe Cytokine Release Syndrome. The CAR T-cells have been shown to also access sanctuary sites such as the central nervous system and eradicate cancer cells. CD19 antigen is expressed by majority of the B cell malignancies and therefore most studies using CAR T-cell therapy have focused on the treatment of advanced B-cell malignancies such as Chronic Lymphocytic Leukemia (CLL), Acute Lymphoblastic Leukemia (ALL) and Non Hodgkin lymphoma (NHL), such as Diffuse Large B-Cell Lymphoma (DLBCL). Previously published studies have shown significant responses with CAR T-cell therapy in patients with relapsed and refractory B-cell ALL. But the durability of remission has remained unclear.
Patients, following treatment with CAR T-cells, develop B-cell aplasia (absence of CD19 positive cells) due to B-cell destruction and may need immunoglobin replacement. Hence, B-cell aplasia can be a useful therapeutic marker, as continued B-cell aplasia has been seen in all patients who had sustained remission, following CAR T-cell therapy. Cytokine Release Syndrome, an inflammatory process is the most common and serious side effect of CAR T-cell therapy and is associated with marked elevation of Interleukin-6. Cytokine release is important for T-cell activation and can result in high fevers and myalgias. This is usually self limiting although if severe can be associated with hypotension and respiratory insufficiency. Tocilizumab, an Interleukin-6 receptor blocking antibody produces a rapid improvement in symptoms. This is however not recommended unless the symptoms are severe and life threatening, as blunting the cytokine response can in turn negate T-cell proliferation. Elevated serum Ferritin and C-reactive protein levels are surrogate markers for severe Cytokine Release Syndrome. The CAR T-cells have been shown to also access sanctuary sites such as the central nervous system and eradicate cancer cells. CD19 antigen is expressed by majority of the B cell malignancies and therefore most studies using CAR T-cell therapy have focused on the treatment of advanced B-cell malignancies such as Chronic Lymphocytic Leukemia (CLL), Acute Lymphoblastic Leukemia (ALL) and Non Hodgkin lymphoma (NHL), such as Diffuse Large B-Cell Lymphoma (DLBCL). Previously published studies have shown significant responses with CAR T-cell therapy in patients with relapsed and refractory B-cell ALL. But the durability of remission has remained unclear.
The authors in this study, treated a total of 30 patients with relapsed or refractory ALL ( included those who had relapsed after allogeneic stem cell transplantation and those refractory to CD19 directed bispecific antibody Blinatumomab), with autologous Chimeric Antigen Receptor (CAR) T-cells (CTL019 T-cells) and monitored response rates, toxicities as well as proliferation and persistence of circulating CTL019 T-cells in the patient’s body. The first assessment was performed 1 month after infusion of CTL019 and 90% of the patients were in complete remission and sustained remissions were noted for up to 2 years. At a median follow up of 6 months, the event free survival was 67% and overall survival was 78%. The authors compared this efficacy data with the FDA approved agents for relapsed ALL such as Clofarabine, Nelarabine and Liposomal encapsulated Vincristine, which have a complete remission of less than 25% with a median duration of response of 4-9 weeks. Persisting CTL019 T-cells in the body is a marker of therapeutic efficacy. CTL019 T-cells proliferated in the patient’s body and was detectable in the blood bone marrow, and cerebrospinal fluid of patients who had a response. At 6 months, the probability that a patient would have persistence of CTL019 T-cells was 68% and the probability that a patient would have relapse free B-cell aplasia was 73%. Severe Cytokine Release Syndrome was noted in 27% of the patients and these patients had a higher disease burden before CTL019 infusion. All of these patients were effectively treated with the Interleukin-6 receptor blocking antibody Tocilizumab. The authors concluded that Chimeric Antigen Receptor modified T-cell therapy against CD19 positive cells (CTL019) was highly efficacious, in patients with relapsed and refractory ALL and was associated with a high and durable remission rate. This technology may be applied to other malignancies, as new antigen targets are identified. Maude SL, Frey N, Shaw PA, et al. N Engl J Med 2014; 371:1507-1517
