
SUMMARY: Immune checkpoints are cell surface inhibitory proteins/receptors that harness the immune system and prevent uncontrolled immune reactions. Immune checkpoints are an area of increasing interest as they utilize the patient’s immune system to reject cancer cells. Survival of cancer cells in the human body may be to a significant extent, related to their ability to escape immune surveillance, by inhibiting T lymphocyte Activation .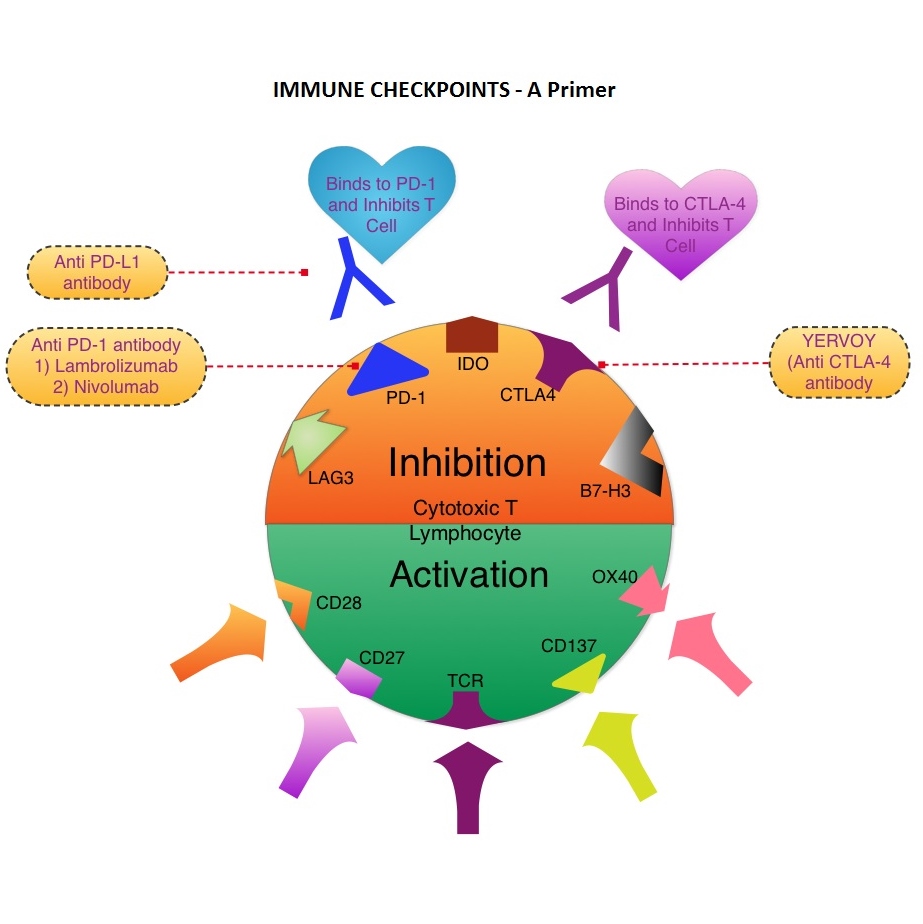 The T cells of the immune system play a very important role in modulating the immune system. EFFECTOR T cells include Cytotoxic T cells, Helper T cells, and Natural Killer (NK) cells, that enable the immune system to destroy cancer cells and pathogens. The REGULATORY T cells however, suppress immune response. Under normal circumstances, inhibition of an intense immune response and switching off the EFFECTOR T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. The mechanism can be compared to a lock and key where the appropriate Ligand (KEY) binds to the Immune checkpoint protein/receptor (LOCK) and activates or inhibits a T lymphocyte. With the ongoing understanding of tumor immunology and the recognition of Immune checkpoint proteins, researchers have focused on the development of antibodies that either target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4, PD-1, IDO, etc. (LOCK) or target the inhibitory soluble Ligands or antigens that are located on the surface of certain cancer cells (KEY) that bind to these Immune check point proteins/receptors. By doing so, one would expect to unleash the EFFECTOR T cells resulting in T cell proliferation, activation and a therapeutic response. The first immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® (Ipilimumab), an antibody that blocks Immune checkpoint protein/receptor CTLA-4, was approved by the FDA in March 2011 and has been shown to prolong overall survival in patients with previously treated unresectable or metastatic melanoma. The next immune check point protein/receptor studied for targeted therapy was PD-1. Lambrolizumab (MK-3475) is a humanized anti–PD-1 monoclonal antibody that demonstrated a 38% rapid and durable response rate and a more than 7 month median progression-free survival in patients with advanced melanoma, regardless of their prior therapy with YERVOY®. Nivolumab, another PD-1 targeted antibody demonstrated remarkable efficacy in a Phase I study with an overall response rate of 30%, median survival of 16.8 months and a 2 year survival of 44%. Based on this provocative data, a combination of Nivolumab and YERVOY® were studied in patients with advanced Stage III or IV melanoma who had received up to three prior therapies.. The idea was to block both the Immune checkpoints, PD-1 and CTLA-4, for improved efficacy. Fifty three (N=53) patients were treated with a combination of these two agents and 33 patients received these agents sequentially. Indeed, the highest response rate was over 50% in the combination group with 30% of these patients experienced a more than 80% response rate at 12 weeks of treatment whereas the response rate in the sequential treatment group was 20%. This preliminary study confirmed that blocking multiple Immune checkpoint proteins/receptors may result in rapid and durable responses in patients with advanced malignant melanoma. Phase III studies are underway to confirm this efficacy data and this concept is also being studied in other tumor types. Targeting/inhibiting the ligands (KEY) and preventing their binding to the Immune checkpoint protein/receptor, is another approach to stimulate antitumor immune response. PD-L1 protein (Ligand) which is often elevated in melanoma tumor cells, bind to PD-1 check point protein/receptor and can inhibit T cells and escape immune surveillance. An investigational PD-L1 targeted (Ligand targeted) engineered antibody (MPDL3280A) demonstrated a rapid response in 26% of the 45 patients with metastatic melanoma and the benefit was more so in those tumors expressing PD-L1. Promising activity has also been seen in advanced renal cell carcinoma. Antibodies targeting the Immune checkpoint receptor/protein or the Ligands binding to these receptors, are being developed, to carry payloads that are lethal to the checkpoint protein/receptor or Ligand. In conclusion, identifying as well as inhibiting certain Immune checkpoint proteins/receptors and/or Ligands that bind to these receptors, may give us new insights in the field of tumor immunology, resulting in better outcome for our cancer patients. Patel JD, Krilov L, Adams S, et al. J Clin Oncol 2013;32:129-160
The T cells of the immune system play a very important role in modulating the immune system. EFFECTOR T cells include Cytotoxic T cells, Helper T cells, and Natural Killer (NK) cells, that enable the immune system to destroy cancer cells and pathogens. The REGULATORY T cells however, suppress immune response. Under normal circumstances, inhibition of an intense immune response and switching off the EFFECTOR T cells of the immune system, is an evolutionary mechanism and is accomplished by Immune checkpoints or gate keepers. The mechanism can be compared to a lock and key where the appropriate Ligand (KEY) binds to the Immune checkpoint protein/receptor (LOCK) and activates or inhibits a T lymphocyte. With the ongoing understanding of tumor immunology and the recognition of Immune checkpoint proteins, researchers have focused on the development of antibodies that either target the membrane bound inhibitory Immune checkpoint proteins/receptors such as CTLA-4, PD-1, IDO, etc. (LOCK) or target the inhibitory soluble Ligands or antigens that are located on the surface of certain cancer cells (KEY) that bind to these Immune check point proteins/receptors. By doing so, one would expect to unleash the EFFECTOR T cells resulting in T cell proliferation, activation and a therapeutic response. The first immune checkpoint protein to be clinically targeted was CTLA-4. YERVOY® (Ipilimumab), an antibody that blocks Immune checkpoint protein/receptor CTLA-4, was approved by the FDA in March 2011 and has been shown to prolong overall survival in patients with previously treated unresectable or metastatic melanoma. The next immune check point protein/receptor studied for targeted therapy was PD-1. Lambrolizumab (MK-3475) is a humanized anti–PD-1 monoclonal antibody that demonstrated a 38% rapid and durable response rate and a more than 7 month median progression-free survival in patients with advanced melanoma, regardless of their prior therapy with YERVOY®. Nivolumab, another PD-1 targeted antibody demonstrated remarkable efficacy in a Phase I study with an overall response rate of 30%, median survival of 16.8 months and a 2 year survival of 44%. Based on this provocative data, a combination of Nivolumab and YERVOY® were studied in patients with advanced Stage III or IV melanoma who had received up to three prior therapies.. The idea was to block both the Immune checkpoints, PD-1 and CTLA-4, for improved efficacy. Fifty three (N=53) patients were treated with a combination of these two agents and 33 patients received these agents sequentially. Indeed, the highest response rate was over 50% in the combination group with 30% of these patients experienced a more than 80% response rate at 12 weeks of treatment whereas the response rate in the sequential treatment group was 20%. This preliminary study confirmed that blocking multiple Immune checkpoint proteins/receptors may result in rapid and durable responses in patients with advanced malignant melanoma. Phase III studies are underway to confirm this efficacy data and this concept is also being studied in other tumor types. Targeting/inhibiting the ligands (KEY) and preventing their binding to the Immune checkpoint protein/receptor, is another approach to stimulate antitumor immune response. PD-L1 protein (Ligand) which is often elevated in melanoma tumor cells, bind to PD-1 check point protein/receptor and can inhibit T cells and escape immune surveillance. An investigational PD-L1 targeted (Ligand targeted) engineered antibody (MPDL3280A) demonstrated a rapid response in 26% of the 45 patients with metastatic melanoma and the benefit was more so in those tumors expressing PD-L1. Promising activity has also been seen in advanced renal cell carcinoma. Antibodies targeting the Immune checkpoint receptor/protein or the Ligands binding to these receptors, are being developed, to carry payloads that are lethal to the checkpoint protein/receptor or Ligand. In conclusion, identifying as well as inhibiting certain Immune checkpoint proteins/receptors and/or Ligands that bind to these receptors, may give us new insights in the field of tumor immunology, resulting in better outcome for our cancer patients. Patel JD, Krilov L, Adams S, et al. J Clin Oncol 2013;32:129-160
Bottom Ad

Advertisement