
SUMMARY: There are presently four Direct Oral AntiCoagulants (DOACs) approved in the United States for the treatment of Venous ThromboEmbolism. They include PRADAXA® (Dabigatran), which is a direct thrombin inhibitor and XARELTO® (Rivaroxaban), ELIQUIS® (Apixaban), SAVAYSA® (Endoxaban), which are Factor Xa inhibitors. Compared to Vitamin K Antagonist COUMADIN® (Warfarin), the Direct Oral AntiCoagulants have a rapid onset of action, wider therapeutic window, shorter half-lives (7-14 hours in healthy individuals), no laboratory monitoring and fixed dosing schedule. The half life of these agents can however be prolonged in those with renal insufficiency. The FDA in October, 2015, granted accelerated approval to PRAXBIND® (Idarucizumab), for those patients treated with PRADAXA® (Dabigatran), when reversal of the anticoagulant effects of PRADAXA® is needed for emergency surgery/urgent procedures, or in life-threatening or uncontrolled bleeding. Unlike bleeding caused by COUMADIN® which can be reversed using Vitamin K or Fresh Frozen Plasma, there are no specific agents presently available, for reversing bleeding caused by the other Direct Oral AntiCoagulants or for stopping the anticoagulant effects of these drugs, in patients who need urgent surgical intervention. 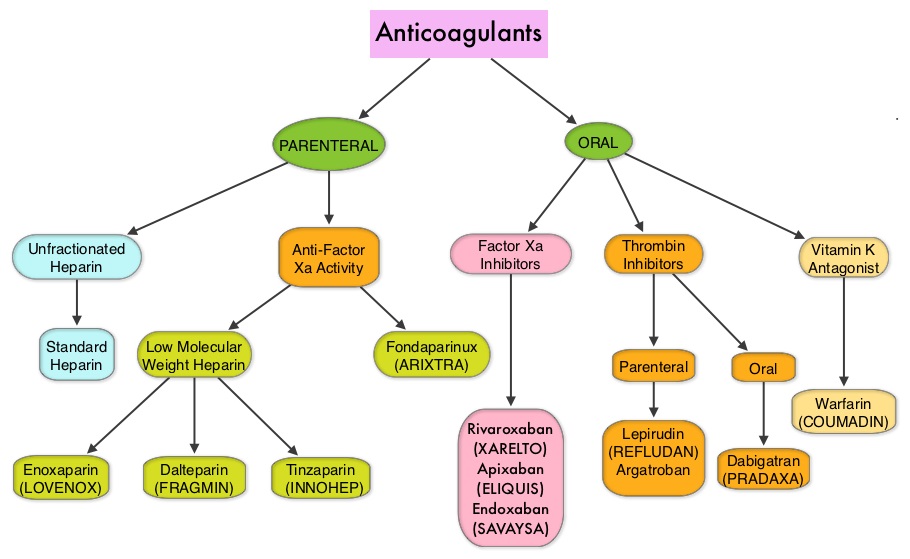
A recently published study has shown that the availability of Direct Oral AntiCoagulants has increased the number of doctor office visits, driven by new visits related to Direct Oral AntiCoagulant (DOAC) use in Atrial Fibrillation patients. It was noted that the utilization of DOAC’s was comparable to the use of COUMADIN® (Warfarin) for Atrial Fibrillation patients (Am J Med. 2015;128:1300-1305).
The discussion by the authors in this article, revolve around a 86-year old female weighing 55 kg, who presented to the ED with persistent Epistaxis. She had a history of Atrial Fibrillation and has been taking XARELTO® (Rivaroxaban) 20 mg, once daily, for stroke prevention for 1 year. She also had a history of peripheral arterial disease and was on Aspirin 80 mg, daily for primary prevention for 9 months. It was noted that the chromogenic anti–Factor Xa assay showed that her plasma concentration of XARELTO® was supratherapeutic. So, treatment with XARELTO® was discontinued. Nonetheless, two days later, the plasma XARELTO® concentration was still within the therapeutic range rather than subtherapeutic, suggesting slow drug elimination. The medical team discontinued her Aspirin and switched her from XARELTO® to COUMADIN® (Warfarin) and discharged her.
Several valuable recommendations made from this case are worth mentioning-
1) Older age and renal insufficiency are important factors contributing to bleeding while on DOACs. Because DOACs are partially excreted by the kidneys, dose reductions are recommended in the event of renal impairment. In a study evaluating the bleeding risk with PRADAXA® (Dabigatran) in the frail elderly, two thirds of patients were older than 80 years, and close to 60% of these patients had moderate or severe renal impairment.
2) Because patients with severe renal impairment have been excluded from phase III studies, DOACs should be avoided in this population along with those patients with extreme body weights.
3) Addition of Aspirin to oral anticoagulants is appropriate for up to 12 months after acute coronary syndromes, percutaneous coronary interventions, or stenting procedures. However, this combination therapy increases the risk of major bleeding by 50% compared with oral anticoagulant use alone.
4) For patients with mechanical heart valves, a combination of Aspirin plus oral anticoagulant may be appropriate. However, only a Vitamin K Antagonist (VKA) such as COUMADIN® should be used and DOACs are not recommended.
5) Although routine laboratory testing of patients taking a DOAC is not required, elderly patients should be closely monitored, with particular attention to renal function. A normal Prothrombin Time excludes supratherapeutic XARELTO® plasma levels, and XARELTO® levels can be measured using anti–Factor Xa chromogenic assays.
In conclusion, even though DOACs have several advantages compared with VKAs, DOACs should be avoided in frail elderly patients.
Optimizing the Safe Use of Direct Oral Anticoagulants in Older Patients – A Teachable Moment. Sennesael A, Dogné J and Spinewine A. JAMA Intern Med. 2015;175:1608-1609
