
SUMMARY: Human Papilloma Virus (HPV) is a double stranded DNA virus and is the most common sexually transmitted infection in the U.S. It was responsible for over 25,000 cancers between 2004 and 2007 in the U.S. and the incidence is rapidly increasing due to changes in sexual practices. Even though the low risk HPV types such as HPV-6 and HPV-11 have been well known to cause benign lesions such as condylomata (genital warts), low grade squamous intraepithelial lesions of the cervix and laryngeal papillomas, the high risk HPV types such as HPV-16 and HPV-18 have been of major concern because of their malignant potential. Since the implication of HPV-16 and HPV-18 in cervical cancer dating back to the early 1990’s, these HPV subtypes have also been found responsible for 45-90% of oropharyngeal cancers and 90% of anal cancers. HPV in tumor tissue can be detected by immunohistochemistry testing for P16 expression and confirmed with HPV DNA PCR. 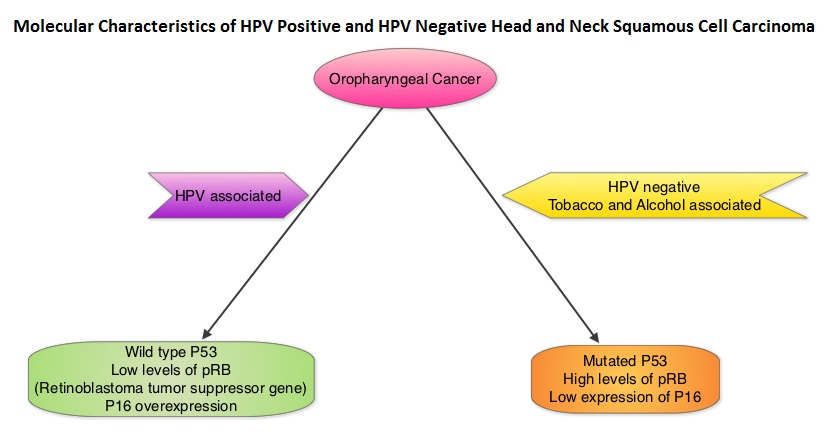 Chronic immunosuppression as seen in patients with HIV and in patients undergoing solid organ transplantation, may increase the risk for HPV infections. Patients with HPV associated oropharyngeal cancer typically are younger males, tend not to smoke or drink and present with poorly differentiated, non keratinizing tumors with basaloid morphology, compared to those with HPV negative tumors. Clinical characteristics of HPV positive oropharyngeal cancer patients with best outcomes include, those with fewer than 10 pack year smoking history and lower tumor stage. Several retrospective trials as well as some small prospective studies have shown that HPV positive oropharygeal cancers when treated with chemoradiation have significantly higher response rates, progression free survival, overall survival and better local and regional disease control. In the TAX 324 randomized phase III trial, patients received induction treatment with 3 cycles of TAXOTERE®, Cisplatin and 5-Fluorouracil (5-FU) or Cisplatin and 5-FU followed by chemoradiation with concurrent PARAPLATIN® (Carboplatin). Even though the 3 drug induction treatment group had superior outcomes compared to those who received 2 drug induction regimen in the intent to treat population, on retrospective analysis, patients with HPV positive oropharyngeal cancer had a significantly longer 5 year progression free survival (78% vs 28%) and overall survival, with an 80% reduction in mortality (HR=0.20, P<0.0001), compared to HPV negative patients, regardless of induction treatment. Other studies have shown that HPV positive patients who undergo surgery alone for oropharyngeal cancer do not appear to reap these favorable benefits, suggesting that the improved prognosis in the HPV positive patients with oropharyngeal cancer is related to chemotherapy and radiation. It also appears that HPV positive patients with oropharyngeal cancer have a better prognosis with treatment when their tumors are P53 wild type and express P16. With regards to EGFR and P16, there appears to be an inverse correlation between P16 and EGFR expression and patients with tumors expressing P16 and not EGFR have a significantly higher 5 year disease free and overall survival compared to those whose tumors overexpress EGFR but not P16. This information may have significant therapeutic implications and studies are underway trying to address this group of patients with targeted and less intense treatments. It should be noted that HPV positive status has a favorable prognostic value only for oropharyngeal primary cancers and not for other cancers of the head and neck.
Chronic immunosuppression as seen in patients with HIV and in patients undergoing solid organ transplantation, may increase the risk for HPV infections. Patients with HPV associated oropharyngeal cancer typically are younger males, tend not to smoke or drink and present with poorly differentiated, non keratinizing tumors with basaloid morphology, compared to those with HPV negative tumors. Clinical characteristics of HPV positive oropharyngeal cancer patients with best outcomes include, those with fewer than 10 pack year smoking history and lower tumor stage. Several retrospective trials as well as some small prospective studies have shown that HPV positive oropharygeal cancers when treated with chemoradiation have significantly higher response rates, progression free survival, overall survival and better local and regional disease control. In the TAX 324 randomized phase III trial, patients received induction treatment with 3 cycles of TAXOTERE®, Cisplatin and 5-Fluorouracil (5-FU) or Cisplatin and 5-FU followed by chemoradiation with concurrent PARAPLATIN® (Carboplatin). Even though the 3 drug induction treatment group had superior outcomes compared to those who received 2 drug induction regimen in the intent to treat population, on retrospective analysis, patients with HPV positive oropharyngeal cancer had a significantly longer 5 year progression free survival (78% vs 28%) and overall survival, with an 80% reduction in mortality (HR=0.20, P<0.0001), compared to HPV negative patients, regardless of induction treatment. Other studies have shown that HPV positive patients who undergo surgery alone for oropharyngeal cancer do not appear to reap these favorable benefits, suggesting that the improved prognosis in the HPV positive patients with oropharyngeal cancer is related to chemotherapy and radiation. It also appears that HPV positive patients with oropharyngeal cancer have a better prognosis with treatment when their tumors are P53 wild type and express P16. With regards to EGFR and P16, there appears to be an inverse correlation between P16 and EGFR expression and patients with tumors expressing P16 and not EGFR have a significantly higher 5 year disease free and overall survival compared to those whose tumors overexpress EGFR but not P16. This information may have significant therapeutic implications and studies are underway trying to address this group of patients with targeted and less intense treatments. It should be noted that HPV positive status has a favorable prognostic value only for oropharyngeal primary cancers and not for other cancers of the head and neck.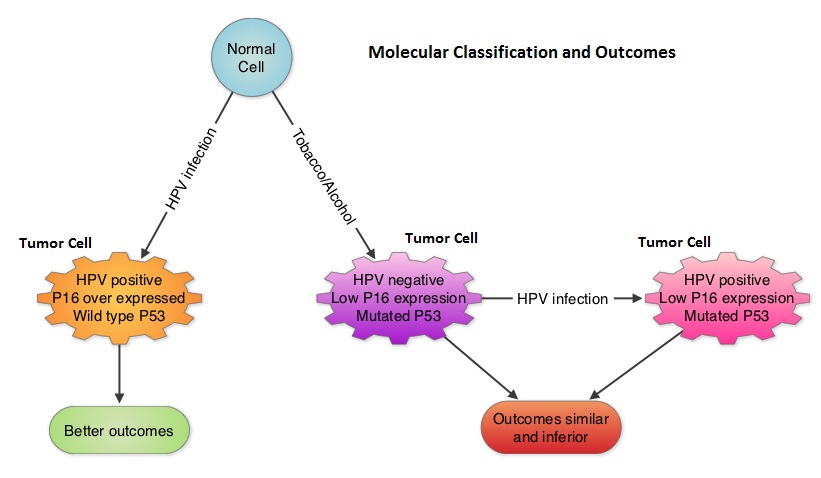
With regards to anal carcinoma, there appears to be a relationship between cervical, anogenital and oropharyngeal cancer suggesting a genital-anal-oral transmission of HPV. Patients with HIV infection have a higher risk of developing HPV associated anal carcinoma and antiretroviral therapy does not decrease this risk. Anal Pap test is recommended annually for high risk patients including those with a history of anogental warts and women with abnormal cervical or vulvar cytology. For patients with anal carcinoma, positive HPV status does not confer a favorable prognosis as is the case for patients with oropharygeal carcinoma. GARDASIL®, a quadrivalent vaccine targeting HPV-6,11,16 and 18 as well as CERVARIX®, a bivalent vaccine targeting HPV-16 and 18 are presently available in the U.S. They are recommended for both females and males at an age as early as 9 years and given as a 3 shot series, to prevent HPV related Cervical Intraepithelial lesions/cervical cancer and genital warts/Anal Intraepithelial Neoplasia respectively. The authors conclude that HPV infection and associated malignancies are preventable and attempts should be made to eradicate this virus. Zandberg DP, Bhargava R, Badin S, et al. CA Cancer J Clin 2013;63:57-81
